The Supreme Court decision in the Asian students vs. Harvardand UNC case may start to turn this around but it’s going to take decades.
1 Like
It’s too bad Rufo and company didn’t get enough traction sooner, because under Trump at the end he had an executive order that nearly killed CRT / DIE stuff since any government contractor would lose funding if they had any of that stuff. So all of a sudden, instead of letting the far left outrage zealots call the shots, the lawyers and the guys making sure the business gets paid said all those diversify / white fragility trainings were on hold and too risky. Many universities, and nearly all good ones, get federal funding in some capacity, so a similar action by the next President could put a serious dent in this.
I am hopeful for a good ruling on the Harvard discrimination case, but worry that racist education bureaucrats will just switch to holistic admissions and no tests, and somehow keep accepting all those unqualified black candidates over the much higher qualified Asian ones for inexplicable reasons.
2 Likes
Finally, a way to correct the imbalance in medical school outcomes. This will do the same thing that the idiotic implementation of integration did to public schools. Now before the HItlerites start calling me Sheets Byrd, I called the implementation idiotic - not the integration.
2 Likes
This is already happening in the California higher-ed system.
2 Likes
The California voters have repeatedly passed no racial discrimination amendments to the constitution (e.g. prop 209) but they are routinely ignored by the Democrat dominated state government and of course the far left University bureaucracy. It is interesting that even in 2020 when Biden was winning California the voters rejected a proposition to overturn the equal rights amendment passed in the 1990s
2 Likes
This kinda reminds me of my experience on a smaller scale in the police academy.
Back in the mid 2000s, the police department I would eventually work for took a very progressive approach towards policing that seemed to work out really well. For its size and budget, it was one of the early adopters to the community policing model. Crime dropped dramatically. It was hailed as a huge success. I don’t think it hurt, and it definitely helped in some ways (more people did come forward with tips on homicides), but there were so many other factors at play from 2000-2009 that no one could really say that community policing (started by the new chief in 2005) was the main driving factor. Prior to the 2000s, we were one of the most dangerous cities per capita in the country, so there was only one direction to go. It was already trending downward before community policing was implemented, and crime went down all over the country during that time.
But along with his community policing policies, the chief completely changed the hiring standards and trajectory of the training for new recruits. He immediately started telling HR that they needed to focus on hiring black officers. The recruiters came back with the unfortunate fact that a lot of otherwise decent black applicants were not passing the background check because of criminal convictions and drug use. So he implemented a policy that allowed for people with misdemeanor convictions and no drug use in the past 3 years to make it through. While at the same time, he started demanding that the training academy relax the physical standards, focus on more on academics, try to keep recruits from quitting, and make sure anyone who didn’t quit, pass the academy. This change was slow, but the by the time I was hired in 2008, the academy had completely abolished the policy of “smoking” the recruits when we screwed up and treating us like dog shit for the first half of our training until we “transitioned” into blue uniforms. We were given blue uniforms the day we started. We also had people in our class that passed even though they didn’t meet some of the “required” physical standards.
The folks in the department that went through the traditional training resented the newer academy classes because we came out much softer. But thankfully, the field training (which is based in answering actual 911 calls for service, not controlled scenarios) can’t be toned down and softened. What that meant was that the shitty cops got weeded out AFTER the academy when they couldn’t actually handle a real arrest, instead of IN the academy when the training officers would have recognized they weren’t going to cut it and pushed them hard enough to quit then. And the rest of the cops got their real training on the back end instead of in the academy.
I guess my point is, we are going to have more shitty medical student interns in hospitals when they finish their two years in med school, no doubt. But they can’t fake their way through operating on someone with a gunshot wound. There are lots of jobs out there for doctors that aren’t actually very good at fixing patients to work in fields where they don’t try to fix patients. The less qualified and dumber med students that are coming through med schools now that only made it in because of diversity policies, if they make it through their internships and still haven’t figured out how to be good at patient care, will likely end up somewhere where their screwup isn’t going to result in someone dying. It will more likely result in poor hospital management or some other administrative snafus. I guess what I am saying is that I’m not too worried about the HBCU grad with a 3.2 gpa someday being the doctor that will perform my kidney transplant. She’ll be somewhere along the line screwing up the waitlist so that 70 year old overweight me gets a kidney a few weeks before some 14 year old kid who should have had first dibs on it.
1 Like
You are being way too optimistic. As they say in the profession, they bury their mistakes.
2 Likes
And if your in Cleveland, and in need of a neuro …
They’re not teaching doctors like they used to.
4 Likes
This is disgusting. Sadly, I plan to live long enough to be a victim of it. Also sadly, I will not be considered as part of a VC. ![]()
I thought I’d follow up on the biased 2017 Commonwealth health care report, since I saw their 2021 report which still agrees the US is terrible since we’re not providing socialized medicine to everyone.
They rank the US dead last in 4 out of 5 categories. 3/5 of these are basically cost. Oddly, the only category we ranked well in was patient care, broadly, while we we given poor marks for cost and accessibility and “equity” which all are just a way of saying poor people don’t get everything for free like these guys want.
Confounding factors used to ding the US on health care quality include
-
high infant mortality rates, which are measured meaningfully differently by country and where the US ranks poorly since we count very premature babies as viable weeks before EU countries (of course lots of those die everywhere, but are counted as miscarriages elsewhere), and
-
maternal mortality rates which aren’t adjusted for racial demographics risk factors (black mothers have higher mortality rates by a lot, and that skews our numbers compared to all these other mostly white countries, although they note France does badly too on this metric, which is unsurprising is you look at their demographics).
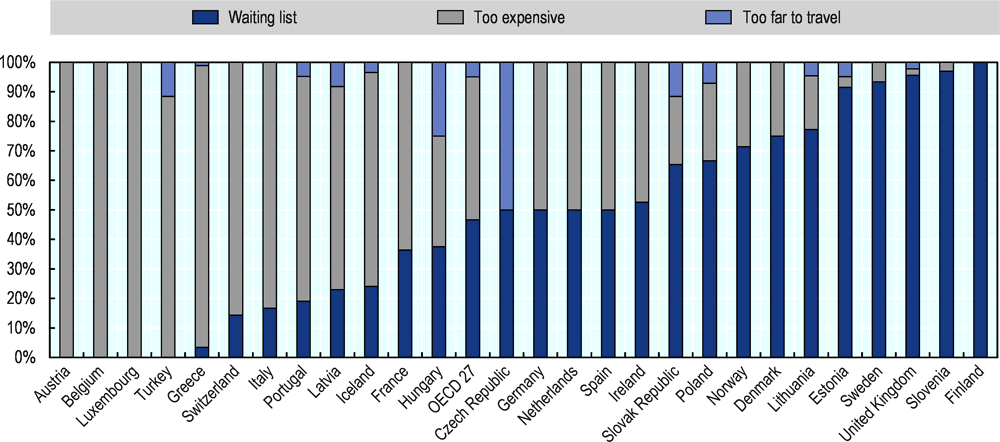
I guess this is what they want - the developed country socialized medicine model where you can’t get care due to wait lists rather than cost. (See blue bar size for richer countries on the right side)
Other things I noticed.
-
their “timeliness” of care metrics didn’t have anything with average wait time, and are skewed towards stuff like having a regular doctor or being able to get emergency care quickly or an answer to an emergency question (all of which were similar most places).
-
you’ll recall the US did very well on care-specific outcomes previously, but not so much on general health. This isn’t surprising to me since the US is much less healthy, ie more fat, diabetic, bad diet, low exercise, etc. so they make up measures like “preventable mortality” and give the US bad grades and count this as a healthcare failing. But care quality is helping the patient you’re given, not the one you wish didn’t need your help. Ok, maybe all the fat people with health issues are a public health failure in the US, but it doesn’t seem right to blame your MD for it (and their appendix 5A does show US leads all countries in recommending better lifestyle choices, it’s just we don’t follow their advice). Maybe we can blame the recent leftist “body positivity” movement (eye bleach warning)?
Stroke Survival
This year’s Commonwealth report does mention
The U.S. ranks last on the mortality measures included in this report, with the exception of 30-day in-hospital mortality following stroke.
so they admit the US is the best country to have a stroke in if you want to live, even if it’ll cost you double. And strokes are the 3rd to 5th leading cause of death, depending if you count drug ODs as accidental and/or include Covid.
Cancer Survival
Cancer, you’ll recall, was another place were timely access to care leads to earlier diagnosis and better outcomes in the US, as well how we offer newer, more expensive and often better cancer treatments than are yet approved by the NHS or similar socialized health bureaucracies that need to control costs. A picture is worth…
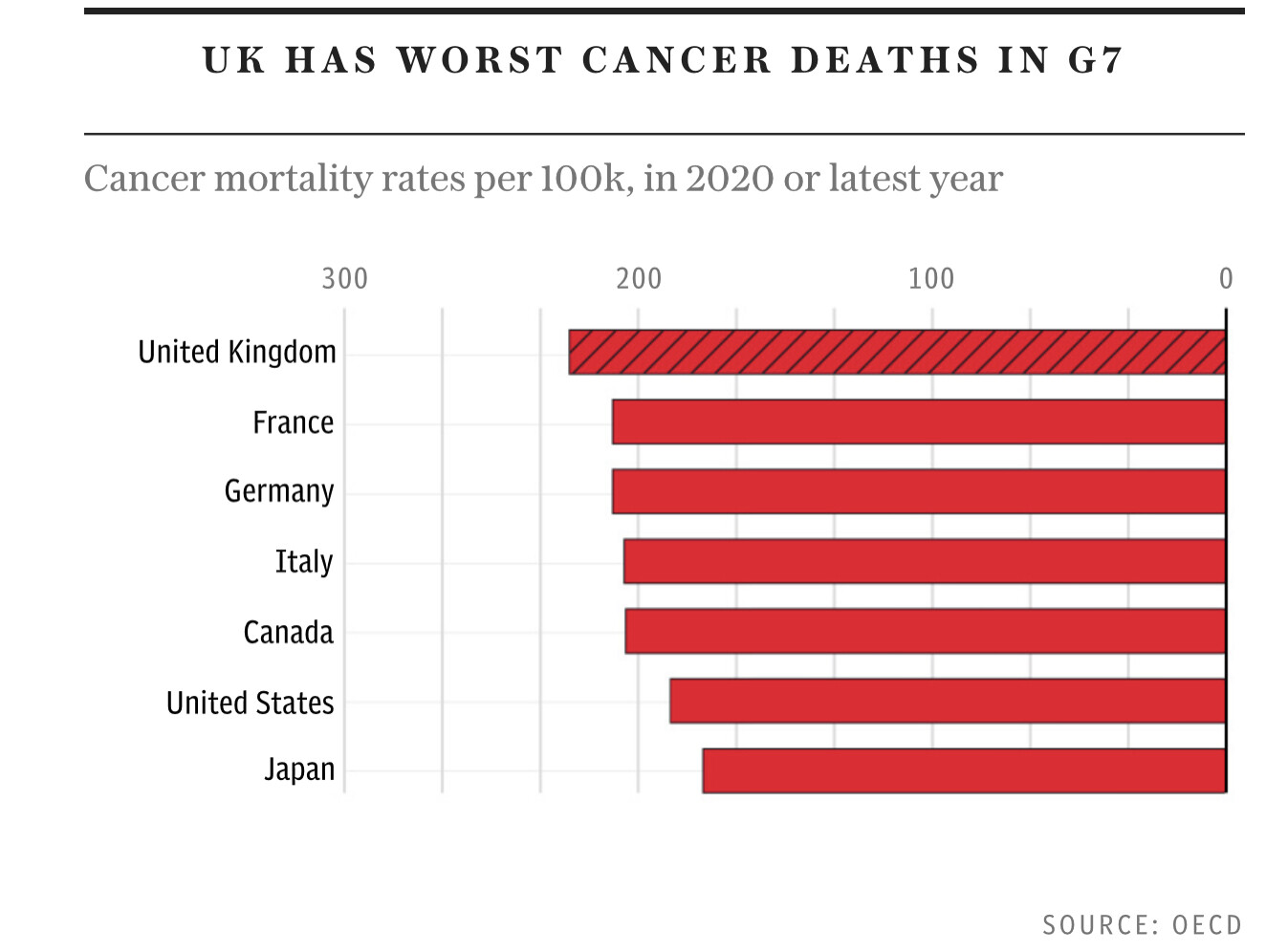
Clearly the US sucks for cancer too. Unrelated I’m sure…
We dropped two OECD measures related to five-year cancer survival rates (breast and colon), because recent data were not available.
the UK had terrible cancer survival rates, which I’m sure are only getting worse due to their long Covid lockdowns and backlog of preventive care screenings.
Some other sources discussing how the US private healthcare prioritizes screening and testing (maybe for liability reasons) and consequently cancers tend to be found earlier and treated more successfully as measured by 5 year survival rates.
Summary
This was a good summary of one of their prior reports, still true today.
The recent Commonwealth Fund study, which ranked the NHS well, has its merits, but it is structurally designed to favour an NHS-style model of healthcare. The study’s limitations are perhaps best, albeit unintentionally, captured by The Guardian’s coverage of the report which stated: ‘The only serious black mark against the NHS was its poor record on keeping people alive.’
3 Likes
Need a kidney transplant? Better start identifying as “black” on those medical forms.
The Organ Procurement and Transplantation Network (OPTN) and the United Network for Organ Sharing (UNOS) are implementing new policies to make skin color a crucial factor in who receives life-saving kidney transplants.
The corruption of medicine continues apace. Black patients are being pushed toward the front of the kidney-transplant waiting list on the basis of something other than need. Racial reparations have arrived in health care, and kidney transplants are just the beginning.
3 Likes
Medical reparations for kidney transplants? Unbelievable!!
I say, get in line. Equal treatment! Didn’t we all get in the line for Covid shots?
1 Like
In progressive states, favored minorities got more access and priority for distribution of life saving vaccines and later antivirals. Whitey should just die to further Racial Justice.
https://www.nyc.gov/assets/doh/downloads/pdf/covid/covid-19-vaccine-equity-strategies.pdf
https://www.cato.org/commentary/why-racial-priority-covid-19-vaccine-distribution-poses-problems
4 Likes
Which are perfectly safe and effective. ![]()
How about quoting the original press release and discussing that instead of just the one-sided hit piece? Emphasis mine:
Also there was a Freakonomics M.D. podcast about this in December. Educate yourself before promoting one-sided reactions without any context.
It sure is unbelievable, because it’s not true.
Doesnt that also mean this has allowed some Black patients to avoid unnecessary treatment for kidney failure?
I dont want this to be my understanding, but I’m failing to see any other conclusion - when studies show that Blacks have a naturally higher level of creatinine, and the eGFR score is based on creatinine levels, there should be a race adjustment of some sort in the score’s formula. It’d seem that eliminating the racial adjustment will mean that Blacks will receive a priority over non-blacks in that they’ll start treatment (and the transplant clock) sooner due to benefit of their natural handicap in the unadjusted formula, at a level of kidney failure where non-blacks would not yet be eligible.
So while I’d agree that it presents more as a “one-sided hit piece”, it’s primary points arent exactly fabricated either. Eliminating the race adjustment doesnt create equality, it seems to facilitate an equal but opposite inequity.
3 Likes
Only if eGFR indeed had a correct adjustment and the lack of adjustment is unjustified. I’d leave that decision to the medical professionals involved in the process, not random commenters on the internet.
Thanks for the link to the podcast transcript.
They go through the details of the estimated kidney measurements and how the estimating function was not designed by a bunch of racists trying to kill black people by denying them transplants. Instead, it was a bunch of Harvard stats people using the expensive, best-in-class kidney measurement techniques (that are too expensive for routine surveillance) and designing a best fit estimation formula. That formula was more accurate according to the statistics if it included black race as a variable, and that made biological sense since the baseline creatine levels vary by race (due to muscle mass varying by race) and so it was useful to know that in judging if a patient’s creatine levels were “high” or not, an indicator of kidney problems.
Said briefly, without this factor, a bunch of black patients who didn’t need transplants would be prioritized for them due to the estimation formula thinking their kidneys were worse off than they actually were. Now the progressive “structural racism in medicine” folks could claim that this meant blacks were being denied transplants, without actually asking the question of whether black patients who needed transplants were being denied them. At the end of the kidney segment in the podcast, the host does ask the progressive crusader if their new formula that removed racial factors was better scientifically.
BAPU: Just purely from a prediction perspective, does the science suggest that including race is more accurate than not including race and including other things that we currently do model?
ENEANYA: The same eGFR equations that were developed in the United States, that statistical accuracy does not ring true when research studies outside of the United States examine Black populations. So there has been a study of populations in West Africa, Black Europeans for instance, and that modifier does not make the equation more statistically accurate in those individuals. So that just tells you that it’s capturing something specific to the United States. I think we have some work to do to see what race is a proxy for.
In short, Yes, in the US where peoples’ kidney function is being estimated and where the US transplants are being decided, race is a useful factor for estimating kidney function. Studies abroad, not relevant to US medicine, suggest this could be due to some confounding factor we don’t understand, but it was a better race-based formula in the US than without, at least until we find that factor and can measure it directly and inexpensively. And, due to Racial Justice politics, it now won’t be used by the transplant boards so they can have a more Just and less scientific approach to handing out kidneys. Progress!
3 Likes
The adjustment didn’t have to be correct. The ‘fix’ to a flawed adjustment isn’t no adjustment; no adjustment can be equally flawed. No adjustment means that more Blacks will be given priority for kidney transplants, despite being healthy and not in need of a new kidney.
And as I said, when creatinine levels are the key to the eGFR result, and Blacks naturally have higher creatinine levels, I’d say it’s pretty obvious that a lack of adjustment is pretty unjustified. More healthy Blacks will receive the unnecessary treatment, to the detriment of everyone with the disease.
3 Likes