2 adults + 4 kids
It’s what would probably be considered a cadillac plan these days. 25/40/250 co-pays, no in-network deductible, out of network coverage included.
This is a myth. There is no free money hiding here. There is a powerful moral case for preventive care but in practice it costs more in extra visits and tests than the savings in serious illness.
A study of Oregon’s Medicaid expansion showed that ER visits went up rather than down. https://www.washingtonpost.com/news/wonk/wp/2016/10/19/more-evidence-expanding-medicaid-increases-emergency-room-visits/
“People covered by Medicaid were more likely to both see a physician at a regular office visit and also go to the emergency room, casting doubt on the idea that people were using health coverage to shift their health care to a primary care doctor.”
There is a lot of institutional inertia around existing inefficient practices (consider coding and billing, or the sheer number of actors involved in filling and administering a prescribed drug), which no model of “who pays” will necessarily make better or worse. Without some reform to the market, this inefficiency and rake-taking will seamlessly transition into inefficiency under any model of who pays for health insurance.
If nationalized healthcare were somehow to overcome obstacles to change and if the US ended up with a system which followed the UK model, then we would see something like:
(1) People generally get pretty good care and never worry about how to pay the bill. Usually urgent issues are handled quickly and correctly and sometimes less urgent issues may require an appointment and some waiting.
(2) People generally don’t declare bankruptcy due to medical bills and are less likely to die of disease which they could not afford to have diagnosed or treated.
(3) People who lose their jobs generally don’t also lose their access to health care.
(4) Private insurance exists and many employers buy private supplementary insurance for their employees; if you say “I have private insurance” at your appointment with your GP you get a faster appointment with a specialist (though not necessarily better care).
(5) As an employee you don’t have to spend days modeling your healthcare plan spend every open enrollment period under your coverage, your spouse’s coverage, the state’s marketplace, and the health-shares alternatives. Nevermind the $, you just gain a lot of time not thinking about it.
(6) Hospitals continue to sometimes provide the wrong treatment and make mistakes; iatrogenic disease will continue to be a major cause of death. Some hospitals will continue to be under-funded and under-staffed and care will suffer in some areas. This will now be blamed on “the government” instead of the fault of individual particular local healthcare monopolies; publicity will call this a failure of the entire system and will demand oversight and changes (which won’t always reliably happen).
Other effects of socialized medicine:
(1) medical expenses will be hidden in other budgets masking the true cost to the government. For example, medical billing costs will be attributed to the tax collection and disbursal bureaucracies.
(2) The associated government bureaucracy will grow exponentially. The British NHS employs 1.6 million people in a nation of 60 million i.e. 1/6 the size of the US.
If the numbers in the two countries are proportional to the population, the US bureaucracy will be about 10 million. Compare this to the approximately current 4 million US federal employees including the military. So the US bureaucracy will more than triple, 4 million to 14 million.
- Expect the availability of advanced medical technology such as CT and MRI scanners, radiotherapy accelerators to drop drastically resulting in long wait times if you need a scan or therapy.
- expect the innovation rate of development of new medicines to drop as the US funds a lot of the R/D by drug companies around the world.
p.s. yeah I know we are debating the wisdom of socialized medicine but I could not resist 
@onenote Medicare does not directly hire doctors to treat patients or run medical facilities. There is no serious proposal placing all medical professionals on the government payroll and taking over hospitals, clinics, etc. Time to turn off Fox News and join us in the real world.
How is the UK’s system funded?
How is the UK managing the structural inefficiencies you mention?
And here I thought Americans go to Canada, Mexico, and Asia for cheaper care.
That article cites a study off the healthcare systems in 11 nations
Canada was #10
UK was #1
USA was #11
Yes Canada has bad wait times. The worst that study looked at. USA has all sorts of problems that I’m sure we’re mostly familiar with.
Plus we pay 2x what anyone else does for our broken system.
Long wait times in Canada doesn’t refute the effectiveness of socialized medicine. Look at the UK in that study.
Speaking basic economics here: Isn’t the current system preventing wait times by denying access to certain people? Have we decided, as a society, that those people don’t deserve treatment? If so, why?
I know quite a few Canukes that lives in the US. Their basic care is fine, but “elective” surgery can be on the waitlist for a while.
A good case study is Taiwan which done a huge switch-over to single payer system from a pay-as-you-go system. Because of the lack of employer paid insurance, their health care cost was low. The cost has now raised quite a bit.
There are a number of demographic differences between countries that make direct comparison of health outcomes difficult.
Also, that commonwealth fund report really downplays health outcomes in their ranking criteria, in favor of nebulous stuff like affordability and equity. You can die for free with no healthcare but if you get treated for various things like strokes or cancer in the UK your odds of a successful outcome are much worse than the US. That’s what I would care about but these commonwealth people have a different agenda.
Even the Commonwealth Fund study in question concedes that, while they ranked the NHS as the number one health system overall, its competence in the small matter of actually keeping its patients alive was the second-worst of any country under consideration.
This is just sophistry and semantics. If your “business” has and can only have one customer–the government, you are a government employee.
“The National Health Service is the closest thing the English have to a religion,” Margaret Thatcher’s Chancellor Nigel Lawson famously once observed.
How true. Remember the absolutely bizarre opening ceremony at the 2012 London Olympics where they had women wearing nurses outfits swooping around on guy wires and other actors dressed in hospital gowns jumping up and down on trampolines decorated as hospital beds. The announcer intoned how “we love our NHS.”
By that definition all Lockheed, Northrop, and Raytheon employees are government employees.
Heard an informative discussion on future of California medical system on radio. The interviewee is Craig Gotwas, a lawyer who makes his living advising companies on how to cope with government regulations for their employees’ medical insurance. Scroll forward to about the one minute mark to get over the show opening stuff.
Comments:
-
Taxpayers in California now fund 70% of all healthcare (UCLA Study: Taxpayers Foot 70 Percent Of California’s Health Care Tab | California Healthline) via Medicare, Medicaid, CHIP, the VA, Tricare, County/Local Health Programs, PPACA Exchanges and state, local and fed gov’t employees. Other states are generally 60% to 65%. So we already have a mostly socialized system
-
Gotwas estimates that if the Democrats’ plan is implemented it will add about 2 million people to the government paid medical system in California
-
His prediction is that this will lead to even longer wait times for services and reduction in quality of the service.
Craig’s website is well worth reading for fact based information on the state of medical system
Interesting. My first reaction is that 70% sounds really really high but then I realized that majority of the people I see at the local HMO are older folks. People over 65 are already covered by Medicare and that older people use the healthcare system way more than younger folks so with that in mind, the 70% number starts to sound possible.
Medicare is ~20% of total healthcare spending. About 13% of the population is on Medicare. So yeah per capita.
Medicaid is almost 20% too. A bit over 20% of the population is on medicaid.
VA, Obamacare subsidies, etc all add up too.
The broad umbrella of ‘government spending’ may also include government employees which is around 12% of the workforce. That might be 12% of it too.
They cited a report that is here :
http://healthpolicy.ucla.edu/publications/Documents/PDF/2016/PublicSharePB_FINAL_8-31-16.pdf
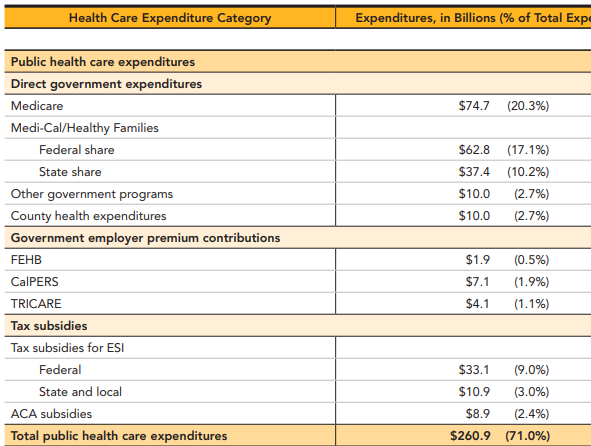
Government employee health insurance spending is included but its only 3.5% of the total
12 % of the “government spending” are tax subsidies for employer sponsored insurance.