There will be no explicit subsidies to get insurers to stay in the market rather they will just keep raising their premiums by double digit percents. The ACA will just be for the those who get subsidies, everybody else will be priced out of the market. For someone making less than 4x the poverty level, premium increases mean nothing, they will pay the same.
1 Like
The really good subsidies, the cost sharing ones ( CSRs), you only get up to 250% FPL. Even over 200%, you only get the Silver 73 plan where you get 73% of your costs covered. The Silver 87 or 94s for those from 100-200% FPL are the really good values assuming you can get decent care from their network.
Over that and up to 400% FPL, you get a partial credit towards your premiums but no help on the deductibles or copays. You will still have thousands of dollars of deductibles and significant premiums that remain after the tax credits. ACA coverage can be unaffordable even if you have it since the out of pocket costs can be quite high aside from the premiums themselves.
The costs to the hospitals is higher beneath Obamacare because the emergency waiting rooms are overflowing with those who’d never had gone to the hospital with their self-caused disease. This results in cost sharing, where patients with actual emergencies (sports, etc.) are extorted to cover the costs of those who have no co-pay or co-insurance abilities - but rely on the deals made between the insurers and the disadvantaged providers. It’d be more profitable to deny service.
Without the requirement, those who choose to not sign up also won’t be found at the hospital - win-win.
No one is required to participate in sports, so their emergencies are self-caused, too, no?
[quote=“PR0N, post:144, topic:31, full:true”]
The costs to the hospitals is higher beneath Obamacare because the emergency waiting rooms are overflowing with those who’d never had gone to the hospital with their self-caused disease. This results in cost sharing, where patients with actual emergencies (sports, etc.) are extorted to cover the costs of those who have no co-pay or co-insurance abilities - but rely on the deals made between the insurers and the disadvantaged providers. It’d be more profitable to deny service.
Without the requirement, those who choose to not sign up also won’t be found at the hospital - win-win.[/quote]
That’s all backwards.
ER visits, particularly uncompensated visits, have dropped since the ACA. The cost-shifting was prior o the ACA, and since the hospitals were no longer receiving payments to help with uncompensated care. Those “who choose to not sign up” are the ones who will increasingly be the ones showing up at the ERs.
Of course it would be more profitable to deny service and kill people. That’s why it’s a federal crime.
1 Like
No. Theres little change in ER use.
Most recent data : https://www.cdc.gov/nchs/data/nhsr/nhsr090.pdf
“Few changes in ER use were noted between 2013 and 2014.”
Hospitals are seeing signficant increases in profit too, since more of the people are insured versus before ACA.
4 Likes
And they’re off !
Maine Community Health Options (MCHO) became the first insurer in the country to sue the Trump administration over millions in subsidies that the federal government cut off in October.
MCHO argues the text of the Affordable Care Act guarantees the cost-sharing reduction (CSR) payments to insurance companies to compensate them for having to accept all patients regardless of their health status. After the payments were terminated, insurers still had to provide subsidies to low-income enrollees, but they were no longer reimbursed.
As an insurer participating in the marketplace, MCHO states it is required to offer CSR plans and is guaranteed to be reimbursed by the government for doing so under Section 1402 of the ACA and its implementing regulations at 45 C.F.R. 156.430.
Centene and Medica are running bottom tier Medicaid-style plans…
If they’re in the ACA marketplace (which they are), they meet ALL the same requirements. You’re falling for the propaganda.
Centene was sued for not providing access to doctors.
1 Like
And the University of Maryland hospital dumped a patient out on the street at night in 30 degree temperatures wearing nothing but a gown and socks.
Anecdotal incidents do not represent a healthcare system.
1 Like
This definitely couldn’t have happened since I was told ER room abuse would go down now that everyone could get Obamacare. I guess you can’t make people use benefits just like you can’t make this lady wear her clothes, which she had in her big bag with her.
Seriously though, it’s not the hospital’s job to provide a homeless shelter under the law. If you come in off the street to the ER complaining of something (or nothing), you get checked out and when you’re found to be drunk / crazy / whatever not an emergency, you eventually get discharged back to the street. ER space and hospital beds are too scarce to waste on people who don’t need that level of care and more people will die if you clog up their facilities with everyone who is cold or wants a free meal instead of people with heart attack or stroke symptoms.
1 Like
Agreed, but the hospital needs to work with shelters etc. to place people like her, not throw them in the street.
Real problem here is an almost total lack of funding/care at the state level for mental illness IMO.
1 Like
This isn’t really an ACA issue, but for a lot of crazy homeless people, you can’t get them to make good decisions (if they could make good long-term decisions, they probably wouldn’t be homeless). If you delivered her to a homeless shelter, she might well have left since they wouldn’t let her drink / keep her pet / do drugs, or she just didn’t like all the rules. If you’re not willing to throw all the crazy people into asylums against their will, some of them will do dumb stuff like freeze to death when there are shelters available. Freedom isn’t always fun to watch, just like people drinking or doing too many drugs and wrecking their lives.
1 Like
It did.
The point was the dumping was as anecdotal as the lawsuit against Centene.
Not in nuthin’ but a gown and socks in 30 degree temps. It’s a federal crime.
Fascinating, your desire to convert GREED into “freedom” for someone else to die.
All this smacks of Darwinism IMO, which the majority of Americans rightly reject.
Well if you don’t like the laws they way they are, feel free to try to get them changed. If you don’t like people making bad decisions, go ahead and ban them from drinking soda or eating at McDonald’s or whatever. For people who make persistent bad decisions, bring back the asylums, but remember they had lots of their own abuses and problems, not the least of which is they couldn’t tell insane people from normal ones so it’s easy to get people you don’t like committed. Some light reading on how that road goes:
Heck, they even thought Sara Connor was crazy. 
1 Like
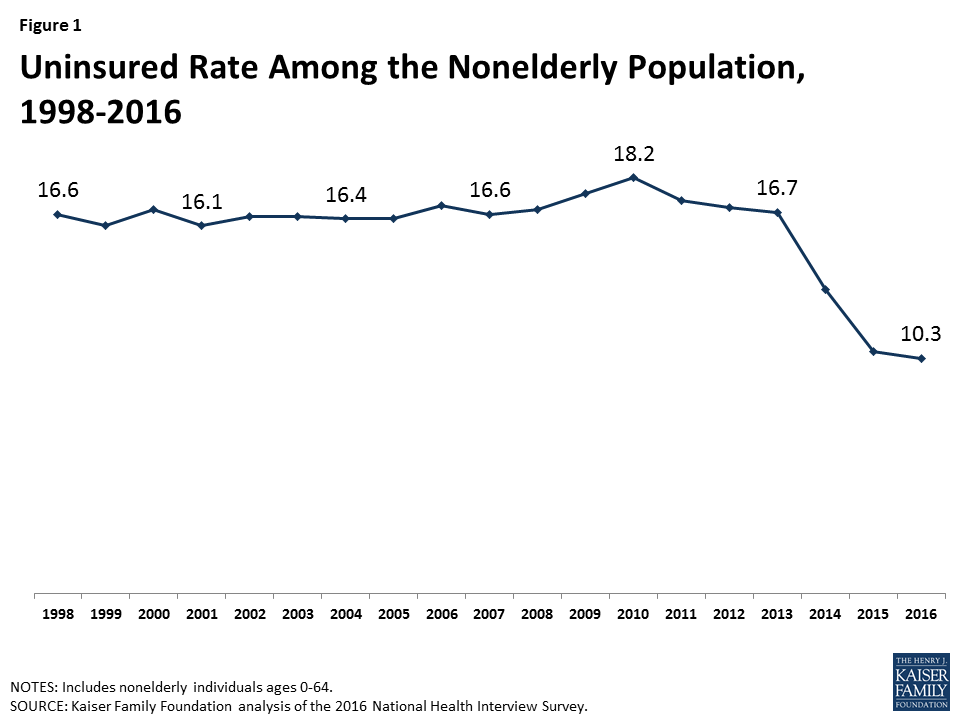
And lest we lose sight of the big picture, remember Obamacare was about increasing the fraction of population with insurance (largely for political reasons IMO), not actually about improving health outcomes per se. And it was a success, in that the uninsured rates have fallen by nearly half, from around 20% of non-elderly adults to a mere 12% (chart below includes children too, but the trends are similar; see the article for details).
But did it actually help health outcomes? Here are the mortality rates, per 100k population, for the same age group 20-64 care of the CDC. You have to put in your own query, but here’s one:
https://wonder.cdc.gov/cmf-icd10.html
(To reproduce, select section 1, group by year, and section 3, age ranges 20-64 each bracket, and years for whichever years you want.)
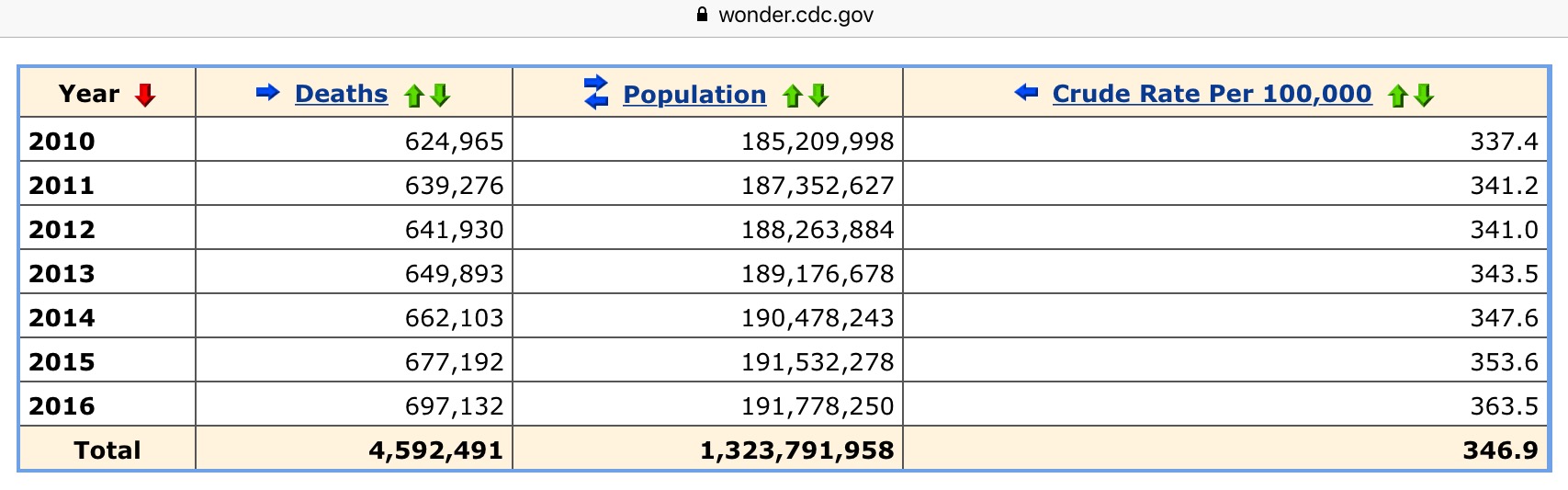
As you can see, non-elderly mortality rates have actually been rising since 2014 when the ACA came into effect, and have continued to rise steadily during the Obamacare period, increasing from around 340 to 364, a 7% increase in the death rate per 100k population. More coverage, but more people dead.
And the rooster crowing causes the sun to rise.
After more than 100 years of continuous increases in life expectancy and reductions in mortality, these suddenly went into reverse [particularly for whites ages 45 to 54] in recent years, due to rapidly rising suicides, prescription drug overdoses, and rising alcoholic liver disease.
And how do you think the poor people who are disproportionately dying from drug overdoses got all these opioids? It couldn’t possibly have been from their shiny free insurance when they realized they could fake some pain to the right doctor and get a nice monthly salary worth of street value drugs to either use or sell to someone who would.
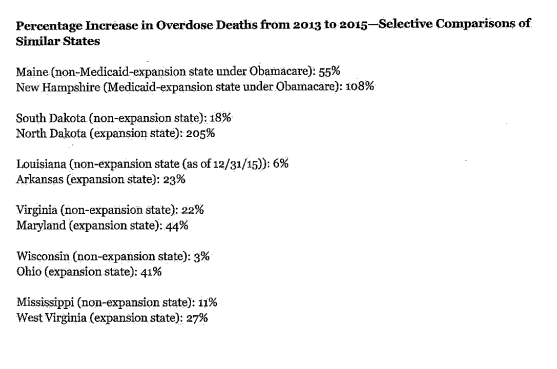
2/3 of the increased death rate above is drug related - this is not a small effect. In addition, by looking at those states who expanded Medicaid vs those that didn’t, you can get a good comparison with lots of data points that show the accelerating rate of the opioids crisis is much higher in places that gave a lot more poor people access to free insurance coverage.
This is not a complicated thesis. We all know what the homeless guy spends your cash charity on, and it’s not food. You can test this yourself by offering the next bum a sandwich instead of cash and see how often you get rejected if not cursed.
https://spottedtoad.wordpress.com/2017/03/27/some-stronger-evidence-that-the-affordable-care-act-worsened-the-opioid-crisis/
Here’s HHS’s comparative selection of states
2 Likes