For some reason, it’s unthinkable to just “give away” anything to all citizens equally and pay all the ongoing bills (mortgages, utilities/debt payments/etc, food) to keep things running a few weeks and to have really fought the virus. That’s socialism.
Just propping up corporations and rich people (who own most equities) is somehow not. A-OK, MAGA approved.
Lots of central banks have already been buying equities directly for a while. The fed is/was specifically prohibited by law from doing something similar. That’s why there’s a roundabout one-step-removed process they created to funnel the money through.
There’s reason for potential concern. But at least for now, I don’t know how much influence the stake gives the government, even if they wanted to use it.
On the other hand, buy low sell high is one of the more realistic ways to offset the costs of coronavirus, and maybe put a dent in the national debt.
Didn’t we see this 10 years ago in the banking industry? I seem to recall the government getting lots of warrants in exchange for “bailout” money, and the whole thing ended up being rather profitable instead of a cost.
A crisis of an industry, yes, but this is a crisis across the board.
IMO a significant difference now is the scope of the crisis, its reach and speed. This is affecting far more people because of the unavoidable lockdowns, travel restrictions, natural fear of many of us to venture out and patronize restaurants, hair salons, even grocery stores. And this isn’t just in the US, or “the West”. It’s everywhere. Poorer countries dependent on tourism are suffering far more than us.
So, this is indeed different… I think.
And yes, I hope the Fed makes a net profit too. Even if it comes out breakeven, it’d be a great success.
That article was about them buying bonds, not stocks. So far, they aren’t buying stocks, they’re just making money really really cheap so you can do it :).
The U.S. Federal Reserve bought $428 million in bonds of individual companies through mid-June, making investments in household names like Walmart and AT&T as well as in major oil firms, tobacco giant Philip Morris International Inc, and a utility subsidiary of billionaire Warren Buffett’s Berkshire Hathaway holding company.
I had mentioned Yellen saying the fed should/might in the future, I think that is what the response was to, just the potential. She did say Congress should authorize it (but there’s other various articles indicating there’d be no difference than the end-run around the law currently being used for corporate bond purchases, and the fed could just do the same thing with equities).
It has come to pass. The curtain has been pulled back. We now learn the real basis for pharmaceutical industry angst over HCQS.
From the WSJ:
Covid-19 Drug Remdesivir to Cost $3,120 for Typical Patient on Private Insurance
Gilead Sciences Inc. GILD -0.04% detailed its pricing plans for Covid-19 drug remdesivir, saying it will charge U.S. hospitals $3,120 for a typical patient.
The drugmaker on Monday disclosed its pricing plans as it prepares to begin charging for the drug in July. The U.S. has been distributing remdesivir donated by Gilead since the drug was authorized for emergency use in May.
Under the company’s plans, Gilead will charge a higher price for most patients in the U.S., and a lower price for the rest of the developed world where governments directly negotiate drug prices. The lower price will be extended to some U.S. government agencies, such as the Department of Veterans Affairs, but not programs such as Medicare that don’t directly purchase medicines, a Gilead spokesman said.
The government price will be $390 a dose, or $2,340 a patient for the shortest treatment course and $4,290 for a longer treatment course.
Gilead said in the U.S. it will charge nongovernment buyers such as hospitals about $520 a dose, or one-third more than the government price, for patients who are commercially insured. That works out to $3,120 for a patient getting the shorter, more common course of treatment, and $5,720 for the longer treatment duration.
SUCH A BARGAIN!!
(not)
ETA
And how many of the doctors conducting those HCQS trials are also Gilead shareholders? According to Sharyl Attkisson, QUITE a few!!
TX scary ICU stats may reflect non-covid backlog of serious health issues, while the covid cases they are seeing now (vs earlier on) are much less senious.
As expected, Federal, state, and local government policy failures in not containing covid19 means there’s a growing backlog of serious health issues (some from precautions about getting the virus) with no end in sight since the virus is now in a runaway growth environment, plus those people are likely to contract covid19 either before treatment or in the course of treatment which makes them more at risk for more serious complications.
– OR –
Everyone will get the sniffles. Let’s just ignore it. It won’t complicate people’s other health issues. Cure is worse than the disease! See? people are needlessly putting off seeking treatment for other issues and they’re making them worse!
Seems like the conclusion is the hospitals aren’t really overwhelmed by the virus (they could make 2-3x more capacity by deferring those nonessential services again if they needed to) and the health impacts of the virus from reopening is likely to be less than earlier given the patients and outcomes they’re seeing.
Neither. The conclusion is that the pending shortage of ICU beds is not a result of current Covid-19 related policy, it’s a consequence of the policies/response over the past 4 months. Had Texas (or wherever, outsides of 3-4 localized “hot spots”) not effectively shut down hospitals in preparation for the onslaught of Covid cases that never came, they wouldnt be facing the current shortage.
I understand that if you reject the premise that our response has been a lot of pointless spitballing with the blind hope that something stuck (in short, “panic”), then there’s no way you can respond to this with anything more substantial than “you’re just being ignorant”. Your limiting the possible conclusions to those 2 options is just your bias, unwilling to accept that there is in fact a lot of rational thinking that goes again what you’ve decided. Plenty of people have said that the measures have been too broad and often counterproductive, and they’ve been saying it all along (not just with the benefit of hindsight).
That’s weird, not what the majority of Drs are reporting and hospital data is showing in TX. ICUs are filling or full. ICU is not “better outcomes” than earlier. Even with “recovery”, the long term damage is bad from the younger patients that go on ventilators.
It’s a much bigger economic loss (aside from the larger loss of life) to have a 35yr old get COPD than for an 80yr old to die, despite resulting in a “recovery” instead of a “death” in the totals.
Except that’s patently false. It’s covid19 patients taking up the bulk of hospital and ICU beds newly filling up now in TX. Unless you think Abbott is now falsifying the state’s data to make it look worse, despite doing the opposite up until now.
One twitter anecdote doesn’t refute the data from across the state.
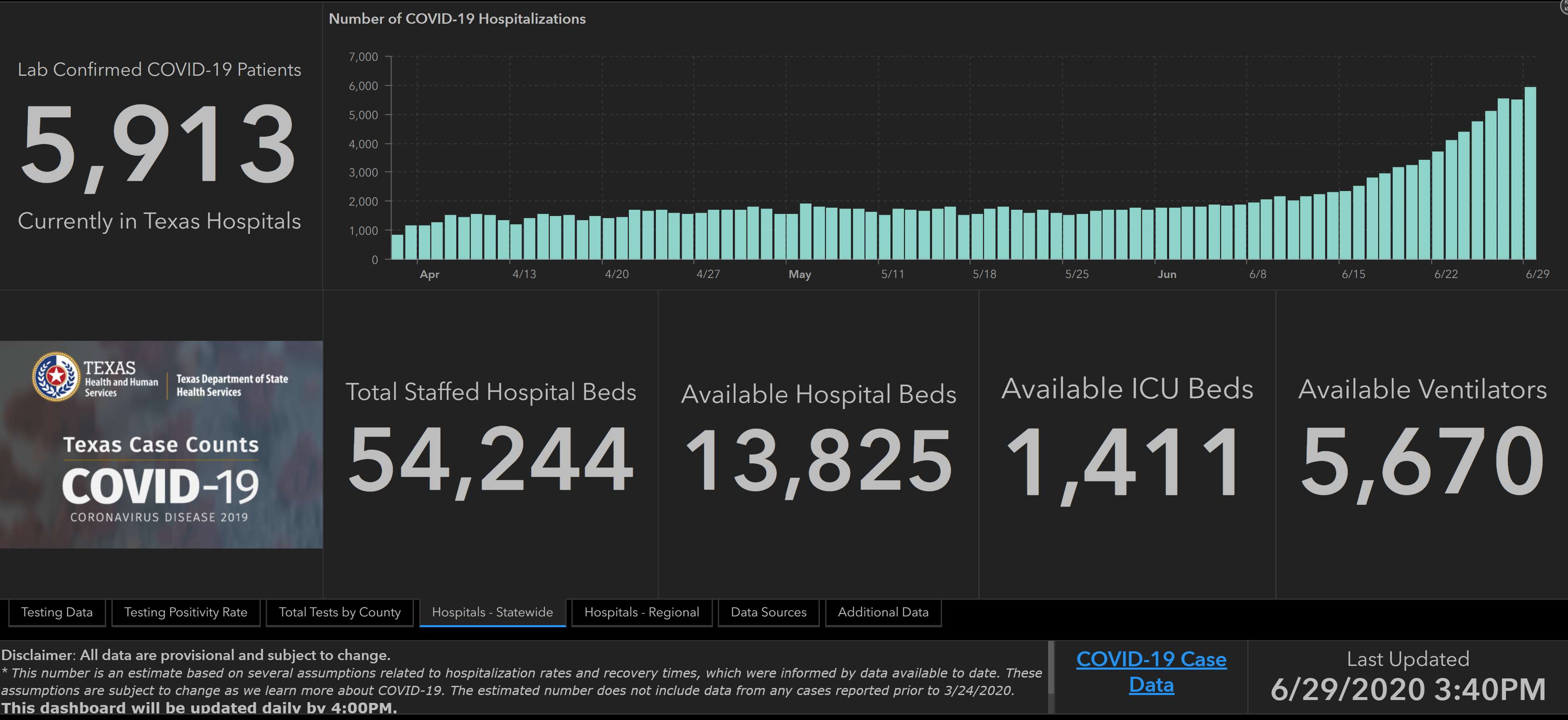
Covid 19 hospitalizations have tripled from ~2k to ~6k in the past 14 days. And that’s only the ones that are lab-confirmed. They double again in about a week (and even if you assume there are no non-lab-confirmed cases taking up more space as well… despite crazy testing shortages – 100s of cars lined up and timeslots filled before 9am across the state), and the capacities are all filled in most areas of the state.
Lol. That’s what you call a lawyer for a “free standing ER clinics chain”?
(and lets not even get into the scams related to the “ER chains”… or screengrabs from a random person’s email viewed on their cell phone… This is way different than “anonymous sources” in News Organizations. Those are verified to at least be who they say they are.)
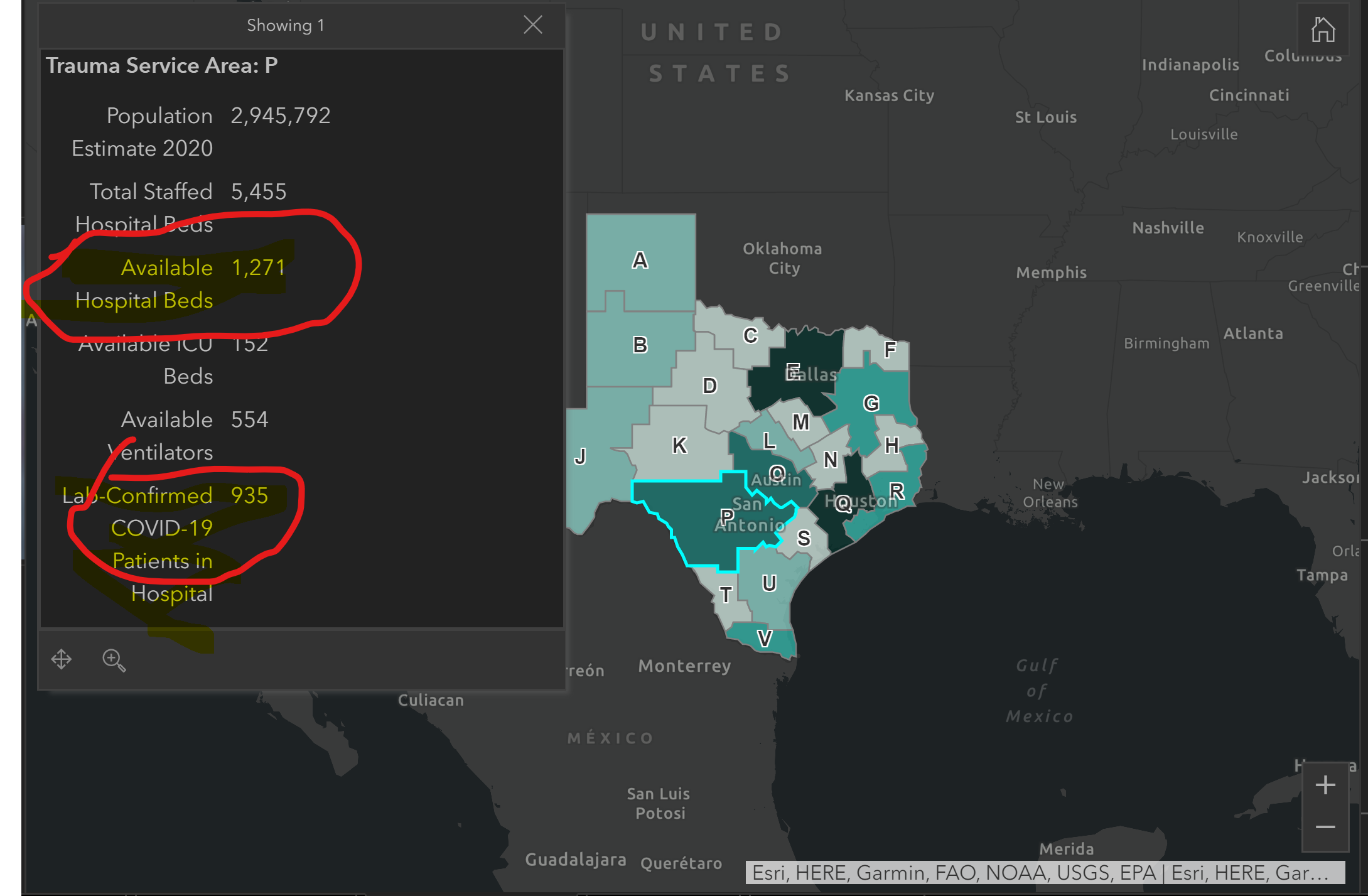
Yes, 935 of 5455 hospital beds is “a bulk” . The volume of hospitalized Covid patents could double and there’d still be available beds remaining.
935 hospitalized also says nothing about how many are in ICU. Even if every one of them required a ventilator, the number could go up over 50% overnight and they’d still have unused ventilators.
Of the increase (“newly filling up”)… It helps to read a whole sentence rather than two words. This number is triple what it was two weeks ago. Triple it again, and there’s still no problem? (and that’s even if you pretend there’s no delay on test results, so the number is not at least 20-30% higher even if there’s only 2 days’ delay.)
We also have had growing testing shortages here the last couple weeks. Those are only the laboratory confirmed cases that are in hospitals. This doesn’t say the data is “wrong”, but it is clearly marked that it is not including all hospitalized covid19 cases.
Oh come on. You clearly said that 935 hospitalized covid patients was a bulk of the 1217 hospital beds with no one in them - you even circled those numbers as being “the numbers”. Otherwise you’re chart was entirely irrelevant.
No, I said if the cases double over the next week, on the course they have been, that would potentially fill up the remaining numbers (this ignores geographic locations – you can’t just use regional or statewide numbers for available beds or ICUs unless you’re gonna ship patients hundreds of miles. Texas is a large state. ~800 miles north-south and ~800 miles east-west. Some areas are already currently at capacity and others are further away from capacity.). That’s why they’re already setting up beds in convention centers now.