I have to type something so the post won’t be empty, but the above deserves repeating, and not just for a needle.
2 Likes
No, that’s a grossly inaccurate paraphrasing. If you wanted to be accurate, you’d say that you understand how some of us have been saying virtually the exact same thing for 12 months now, but were belittled and dismissed for ‘denying the science’. Until suddenly it became “the science”, and now it’s ok. And thus it’s pretty assinine to expect anyone to just abandon what they think and defer to “the science”, when there’s decent odds that in a few months what they think will be “the science”.
It’s the same crock of crap as all this “figuring out how to reopen schools safely”. As if there arent a slew of schools that have been reopened for 6 months already.
5 Likes
You’re pre-cogging the global warming/cooling (whatever it is this decade) debacle. Well, it would be a debacle if reported in a way that was Kardashianable.
1 Like
Yes, schools in my area have been open since 10/20. Teachers vaccinated and all>16 starting 3/24!
They’ve been saying this in Chicago for over a decade. ![]()
2 Likes
No, everyone doing their own thing provides little to no mitigation benefit… Saying for the past 12 months to ignore the public health guidance and “resist” is not following the science.
A CDC recommendation to “just do what you want” doesn’t work to mitigate community spread. Yes, they take multiple factors and decide on the guidelines. Yes, the guidelines can change as the situation changes… The situation is different now than it was 3, 6, 12 months ago.
2 Likes
Yes, 12 months ago was March of 2020. Then, 6 feet was the minimum to prevent killing your friends and relatives. This is March of 2021. Now, 3 feet is cool. Obviously, the Chinese Communists have a thing for even numbered years and made their virus stronger for 2020.
That is the only difference between 2020 and 2021, right? ![]()
Perhaps not. But it is the American way, and has been since our founding:
fed•er•al•ism fĕd′ər-ə-lĭz″əm, fĕd′rə-
- n.
A system of government in which power is divided between a central authority and constituent political units.
The “central authority” is our Federal government. The “political units” are our individual American states.
This system might not make sense to you. But one size does not fit, or suit, all. Not in America.
2 Likes
Not in the America that you remember. BUT … those kinds of ideas are wrong-think, and will eventually be deemed racist or anti-alphabet or hate speech of some form, and then outlawed. ![]()
Feel free to shout from the mountains, but be prepared for the hate that gets shouted at you.
1 Like
My roots go far too deep for such as that to bother me. When young it was my great privilege to associate with many Americans who were born in the 1800’s. The comparison with what is out there today is stark, and most assuredly not in the latter’s favor.
1 Like

If you were talking about transmission of different mutated strains, I could agree since some strains are more contagious than others. But otherwise viral transmission probability for a single strain doesn’t change with time.
The circumstances may be different but it does not change the fact that - with identical mitigation measures - 3ft (or 6 ft) is no safer or riskier now than it was 12 months ago for COVID-19. The shift is purely based on a decision on the economical benefits of reduced distancing, not on the science of viral transmission.
1 Like
Thanks for the mansplaining. That was really informative.
2 Likes
Mitigation efforts like social distancing aren’t an individual measure but the community at a whole. Current conditions do affect what’s reasonable. We now have a large portion of those most vulnerable to immediate mortality vaccinated, and the vaccines are exceptionally effective at preventing death from all the currently known covid variants and reducing hospitalization. Aside from the raw numbers of people vaccinated, many have been infected and have “recovered” so they will have some resistance for reinfection (except to the SA variant. And the resistance will likely fall off – TBD when but we’re at a year past the early infections already). Both of these factors reduce the community transmissibility.
Unknowns are also a risk, and new information is only collected through observation. 12 months in, risks to children appear to be uncommon and they seem to less easily spread the virus between themselves. They do easily spread it to their whole households after becoming infected. But as already mentioned, many of the more vulnerable have been vaccinated now. Do you not agree that all of these affect the risk calculation? It is not exactly the same now as a year ago…
I don’t personally claim 6ft or 3ft is reasonable or necessary for kids or for everyone else. Neither erects a magical forcefield that stops all transmission. Both just reduce it. Everyone indoors can be infected regardless of distance, it’s just less likely the more distance and air circulation to reduce viral concentration in the air by the time it reaches the uninfected person from the one who is contageous.
The CDC decided what was/is a reasonable and judicious approach warranted by current conditions. As a member of society who is not specialized in epidemiology or formation of public policy (other than my vote for representatives…), I defer to those who are. Not white nationalist talking heads on TV, random posts on Facebook, tweets, or my own 5 minute assessment.
2 Likes
Always happy to oblige, ma’mm. ![]()
Ha. I drove out of state to get “it” and it was over so quickly.
2 Likes
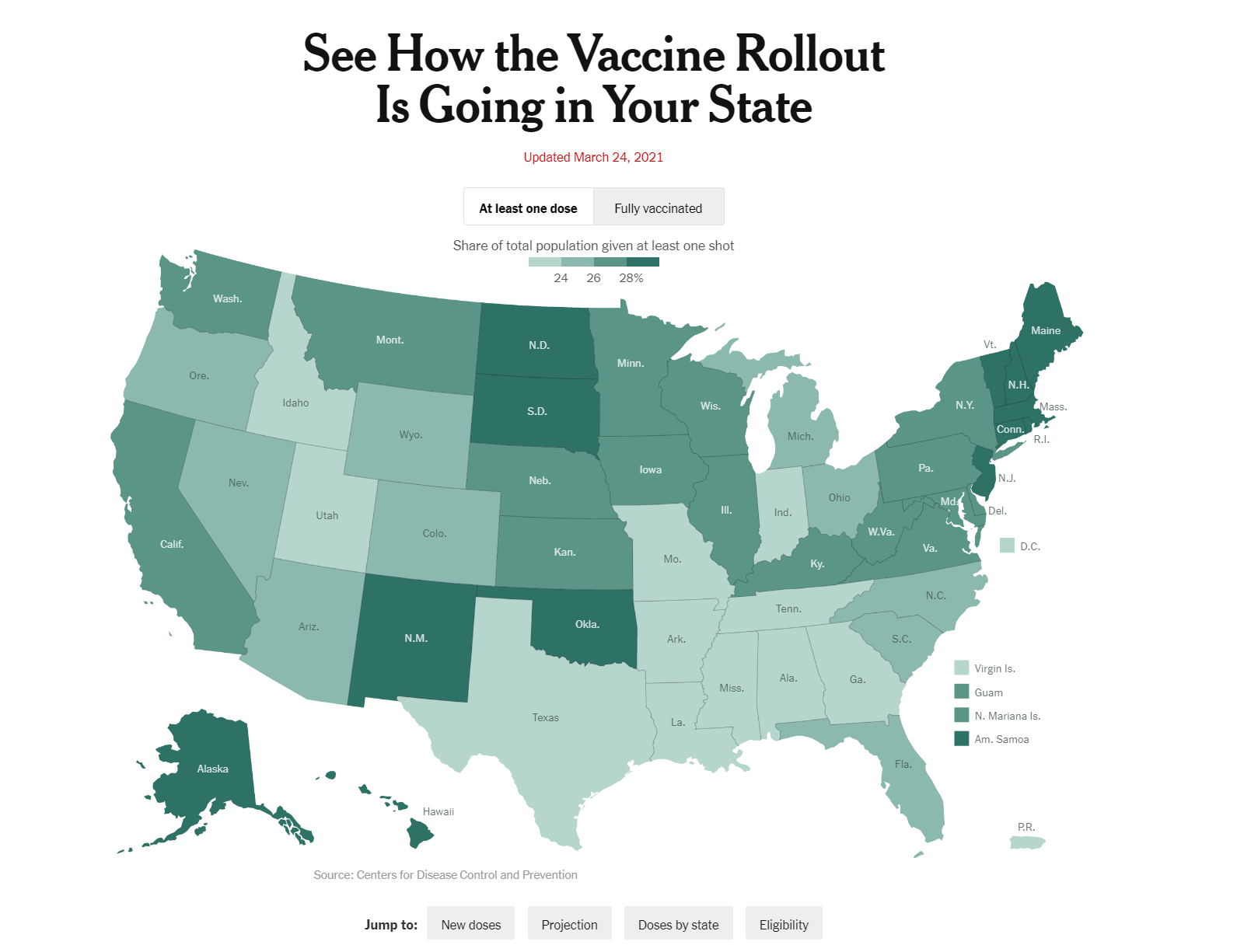
So in an analytical perspective, what’s the cause of the discrepancies in availability between states.
First obvious one may be population age. If you are in a state with an older population, it makes sense that it would take more time to become available to younger population than in a state with younger population.
But that leads to my second reason which would be erroneous allocation which as far as I understand is handled at the federal level. States with older populations should have received higher allocations to account for that fact. But as far as I could read allocation was pretty opaque. Early January, Azar made the allocation based on number of people 65+ vaccinated in each state as an incentive for states to accelerate distribution. That could have amplified issues where if a state was slow to start distribution, they’d also end up being penalized by lower allocations. Is that allocation scheme still in effect or was it changed by the Biden administration? If not that could explain why the states that did a good job at vaccinating people 65+ are flush with doses so that they can allow every adult to be eligible by end of March.
Finally, there is distribution strategy which is solely the purview of each State. That one can clearly lead to discrepancies. If you designed your distribution so that you don’t move down eligibility in age until say 70% of the previously eligible people are vaccinated, then you risk having wasted doses as eligible people who don’t want to be vaccinated are sitting it out while ineligible people who’d want to be vaccinated cannot receive them. The responsibility for good/bad handling of that part is clearly on those in charge at the state level.
But how do you figure if the discrepancies are mostly due to state-level distribution vs. federal allocation scheme? I’m leaning towards some states rolling out distribution better than others but it seems clear to me that federal allocation scheme may have amplified early distribution discrepancies.
AZN has to apply for EUA. Not the other way around. Though, you’re probably right that they know they’ll be told to take a hike as it stood.
Seems like CA and NY is lagging quite a lot. NY looks like a real laggard vs. New England. NJ looks like it’s going well. Mind boggling how poorly run some of these are, vs the others. It’s quite fortunate that the federal govt didn’t decide to somehow run it all themselves.
Some states allow it, and I’ve seen states count seasonal residents in as well.
My preferred vaccine will be Moderna. They, together with JNJ and Novavax, are already developing a variant booster shot.
Will turn down the JNJ and AZN even if offered. Even if I had already rolled up my sleeve.
Fortunately was lucky enough to secure an appointment soon enough of what I was looking for. Was also just invited to signup, but may wait for my preference.
?
Some states being forced to open up to everyone signing up earlier because they are unable to get the higher risk groups actually vaccinated is not a positive indicator…
3 Likes
Oy! You been talking to my first ex-wife? ![]()
1 Like